
Introduction
The previous three courses in this five-part series have discussed pediatric feeding. Part 1 was an introduction to typical feeding development. Part 2 focused on prematurity and the co-occurring conditions that influence feeding development. Part 3 covered constipation, how it can influence feeding and how it can be influenced by feeding. In this course, Part 4, we will discuss congenital heart disease and how it relates to overall feeding and development.
Not surprising, the incidence of feeding problems is higher in the population of children with developmental disabilities. Congenital heart disease is implicated in negatively influencing feeding skills and negatively impacting neurodevelopment. Regardless of whether you're doing feeding intervention or not, it has applications for development in general. The diagnosis of congenital heart disease is very important when thinking about your clientele because it does coexist with a number of other diagnoses.
Disclosures & Learning Outcomes
My disclosures include receiving a salary for my work as an associate professor and a director of clinical education at the University of Louisville. I also received a stipend from SpeechPathology.com for presenting this course.
The measurable objectives for this course include describing three characteristics of congenital heart disease, describing three congenital heart disease diagnoses, and identifying three ways congenital heart disease impacts feeding and/or development. If we don't fully discuss one of the diagnoses that a child on your caseload has, take the time to research it before working with the child. The additional information will be a tremendous help as you're working with that child and family.
The Normal Heart
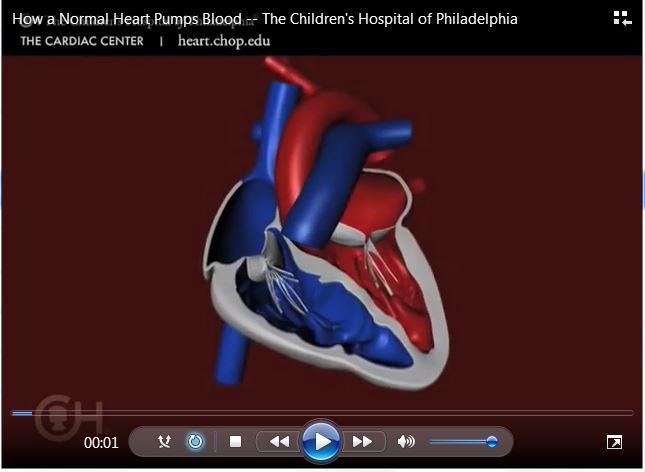
In the normal heart, the left atrium fills with oxygenated blood from the lungs. The left ventricle helps push that oxygenated blood to the body via the aorta. The right atrium fills with blood from the body, which is deoxygenated. Then, the right ventricle helps push that blood into the lungs for oxygenation. There can be deficits in any of these areas and in more than one of these areas, which can be catastrophic for a child, their feeding, their development and their family.
The Heart Valves
Again, the aortic valve is pushing that oxygenated blood out to the body, which is absolutely necessary for function. The pulmonary valve takes the deoxygenated blood to the lungs and gets the oxygen back into the blood. The mitral valve can actually be involved in some of the anomalies that I will be discussing. The mitral valve is the connector between the left atrium and the left ventricle, and the tricuspid valve is the connector between the right atrium and the right ventricle. So all of this is incredibly important.
Blood Flow – Super Simplified
In terms of blood flow, the right side is getting all the blood that needs to get oxygenated. The left side of the heart has all the oxygenation and it needs to get that out to the blood and the body, so that the cells can get what they need. Before each heartbeat, the heart fills with blood, the muscle contracts and moves the blood along. Fortunately, Children's Hospital of Philadelphia does a beautiful job of putting educational videos online and I have a video that I've been given permission to show.
How the Heart Feeds the Body
Keep in mind that the oxygen is going to the cells. The cells in the body use that oxygen and make carbon dioxide. The carbon dioxide is carried away in the blood vessels. In the lungs, the carbon dioxide is removed through exhalation. However, with some children that doesn't happen efficiently and can cause multiple problems.
When the Heart Doesn’t Work Well
When the heart doesn't work well, the heart and the cells don't get what they need. The carbon dioxide doesn't get expelled and everything in the body has to work harder. This is going to have implications for everything; particularly feeding and nutrition. So those very basic, necessary bodily functions are going to be impacted.
Congenital Heart Disease (CHD) Facts
Congenital heart disease is the most common birth defect. It occur eight in 1000 births. It's usually diagnosed in early infancy or early childhood simply because of the ramifications it has. About 25% of infants with congenital heart disease will require invasive treatment during the first year of life. That will clearly impact feeding because that is a very critical period for the infant to bond with their caregivers, to feel homeostasis, to feel attachment, to be able to explore and learn about feeding after about four months when it is no longer reflexive. About 25% of infants are receiving a lot of negative, invasive treatment in that first year of life.
Common Early Symptoms of CHD
Common early symptoms of congenital heart disease include slow feeding, very slow breathlessness and irritability. It's very frustrating for an infant to be hungry and not be able to eat efficiently. Pallor, sweating and failure to gain weight are also common early symptoms.
The nutritional implications are that infants with congenital heart disease may be taking in as many calories as another infant with no congenital heart disease, but his use of those calories and that energy really requires him to have more calories which is very difficult for him.
Common Early Signs of CHD
Some common early signs of congenital heart disease are cyanosis, which is bluish or purplish discoloration because the tissue near the skin’s surface is low on oxygen. Tachycardia is when the upper and lower chambers of the heart are beating too fast and the infant has to work much harder to keep up. This will clearly impact feeding. Tachypnea, or rapid and shallow breathing, can occur due to too much carbon dioxide in the lungs. This results in the brain thinking that it needs to pick up the pace of respiration to try and fix that imbalance. So the infant is trying to suck, swallow, breathe, but instead all they can do is just breathe quickly. Cardiac Murmur is when there is turbulence or disturbance in the normal sound a heart makes when the valves are closing. Another sign is cardiomegaly which is when the heart becomes enlarged because of some of the symptoms of the underlying disease. The last early sign of CHD is cardiogenic shock that can occur when the heart fails to pump and fails to pump adequately. When that happens, circulation and metabolic needs are not met. Again, these are happening during early childhood infancy.
Cyanosis presentation. This is the bluish discoloration of the skin and oxygen saturation is less than 85%. This is the most serious sign of cardiac anomaly. Typically, we like to see oxygen saturations at 95 to 100%. That tells us that 95 to 100% of the red blood cell that have passed through the lungs should be full of oxygen that is needed to feed the body and “be able to feed,” if you will.
Classification of CHD
The classification system of congenital heart disease has two classifications. The first one is Cyanotic CHD which involves decreased pulmonary blood flow or mixed blood flow, and the diagnoses and specific heart problems are broken down that way. The second classification is Acyanotic CHD which is associated with increased pulmonary blood flow and obstruction of blood flow.
Types of Cyanotic CHD
Let’s look at the types of cyanotic congenital heart disease. The types that have decreased pulmonary blood flow are Tricuspid Atresia and Tetraology of Fallot. The types that have mixed blood flow issue are:
- Transposition of the Great Arteries where the pulmonary artery is on the left side and the aorta is on the right side which is completely backwards
- Total Pulmonary Venous Return
- Truncus Arteriosus
- Hypoplastic Left Heart Syndrome
Tetralogy of Fallot (ToF). Tetralogy of Fallot is a defect that involves four problems. (It’s important to understand that just because a child has one diagnosis that does not mean that's the only heart diagnosis they may have. They may have others and that gets extremely complicated.) The first problem is that there is a hole between the two lower chambers of the heart which is basically a ventricular septal defect. The hole causes a leakage of blood; mixing oxygenated blood with deoxygenated blood. The second problem is an obstruction from the heart to the lungs so the blood is not oxygenated adequately. The third issue is the aorta lies over the hole in the lower chambers so it actually looks like the aorta is coming out of both ventricles when it really should be coming out of the left side. The fourth problem is with the muscles surrounding the lower right chamber becoming overly thick, which really makes the individual have to work hard.
Management of ToF. Looking at the management of the Tetralogy of Fallot, if the child's oxyegen is in a safe range, then the medical team may wait on management. But if oxygen is critically low, then they are going to provide the hormone, prostaglandin, to keep the patent ductus arteriosus (PDA) open to increase blood flow. Even though the deoxygenated blood and oxygenated blood are mixing, that’s better than the infant not getting any oxygenated blood.
If the oxygen levels are adequate and there's only mild cyanosis, the infant may go home after the first week of life. They'll have a complete repair at approximately six months of age. If the stats decline for oxygen, they may have to do surgery earlier. At six months of age, we are typically introducing solids and purées. So, this certainly has massive implications for feeding.
Surgical Repair of ToF. Surgical repair of ToF involves closure of the VSD with a synthetic Dacron patch so the blood can flow normally from the left ventricle to the aorta. The resection of the pulmonary stenosis in the right ventricle will be completed so the person can actually get the blood to the lungs in an efficient fashion, and anything additional that needs to be repaired will also occur at this time.
Survival Rate of Infants/Children with ToF. The survival rate of infants and children with ToF is really good. 95% of infants will successfully undergo that surgery. They actually have very good long-term outcomes. They may continue to have a leaky pulmonary valve so sometimes some of that blood will back up and flow back into the right ventricle. But overall, they have really good outcomes medically. However, these infants/children may also need a follow up intervention if that right ventricle pulmonary valve needs more work.
In regards to feeding, the course of action for each child will be very different because ToF is also part of a lot of different syndromes. Therefore, there will be multiple factors to consider.
Hypoplastic Left Heart Sydrome (HLHS). I always talk about HLHS when I am teaching anything on hearts and feeding, and I will tell you why in a moment. HLHS is when the left side of the heart does not form correctly and there may be a co-occurring atrial septal defect. This affects the ability to pump oxygen-rich blood to the body. It can be diagnosed in utero or in the first few days of life. Later, I will share a case study of a child with HLHS that will demonstrate the feeding implications for this heart defect.
Here is another video from CHOP that will give a quick visual: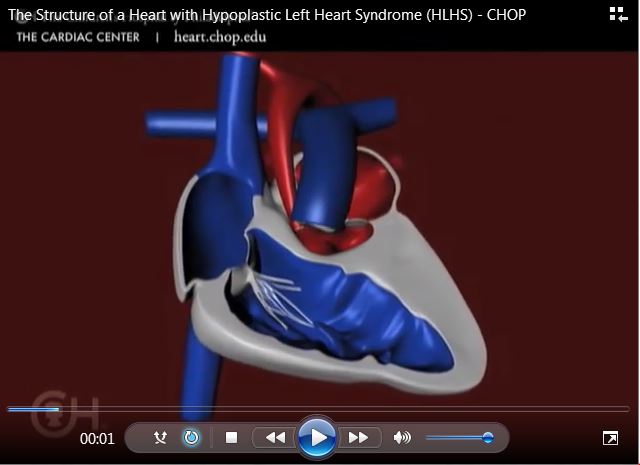
If you're interested, Cincinnati Children's Hospital also has a really good video that's a little bit more detailed, but for our purposes in this course, I did not want to take that much time.
Management of HLHS. This is where we can really see how this is impacting feeding and development. Medications can be used to help strengthen the heart muscle. They can be used to lower blood pressure, get rid of extra fluid.
Nutrition is also used to manage HLHS because, again, many of these children are unable to use the calories that they take in very efficiently. Even if they are taking in 800 calories a baby who doesn’t have HLHS who is also taking in 800 calories is going to be able to use those calories more efficiently. Babies with HLHS have a lot of energy needs.
It’s also important to note that surgery for HLHS is in three stages. It occurs within the first two weeks of birth and that is the main surgery in which they're actually reconstructing the aorta that takes all the oxygenated blood to the body. The next surgery is the Bidirectional Glenn shunt that occurs around four to six months or three to six months of age. That's about the time when we introduce purées and solids to many infants. Then the Fontan Procedure occurs between 18 months and three years.
We have to keep in mind that these infants are having invasive surgeries at least three times. There are, potentially, multiple hospitalizations which can be very negative experiences impacting the child, the family, homeostasis and attachment, as well as a myriad of really serious medical problems.
Survival rate of infants/children with HLHS. What are the survival rates? Surgery is not curative for this disorder and there are lifelong complications that can exist. The survival to one year of age is only about 55.2%. The survival to eight years is only about 50.4%. This is the lowest chance of survival across multiple ages compared to children with any other birth defects studied. So if you have a child on your caseload who has this disorder, you have a child who's been through a tremendous amount. It would not be surprising, then, if they are not extremely happy about eating.
Acyanotic CHD
Looking at acyanotic congenital heart disease, when there is increased pulmonary blood flow, you will see:
- Atrial Septal Defect (ASD)
- Ventricular Septal Defect (VSD)
- Atrioventricular Canal Defect
- Patent Ductus Arteriosus (PDA)
ASD and VSD are very common in children with Down syndrome and are the most frequently occurring.
When there is an obstruction of blood flow from the ventricle, you will see:
- Pulmonary Stenosis
- Aortic Stenosis
- Coarctation of the Aorta
Ventricular Septal Defect (VSD). This is one of the most common heart problems in children with Down syndrome. The walls that form between the two ventricles don't fully develop. There can actually be more than one hole in those ventricles. The blood flows from the left ventricle through the defect into the right ventricle and into the lungs. So if you're not getting efficient use of your blood, there will be excessive blood pumped in the lungs which creates a lot of extra work. Ventricular Septal Defect occurs in 42 of 10,000 individuals and is usually diagnosed after birth.
Management of VSD. Management is accomplished with medicine and that medicine can be for symptomology. Nutrition is very important because these types of disorders result in the child needing more calories and they can't even take in the calories they normally need even without the VSD.
Surgery may or may not occur. It will depend on the size, the problems resulting from the defect, and it may even close spontaneously. So it's not always something that is going to require surgery.
